I struggle with the ADAURA trial. Like many patients, I struggle with treatment decisions and depend heavily on guidance from my doctors. Knowledge, experience, access to research and cutting-edge treatments are all important in providing the best care, but physicians must believe that the patient’s spirit, family, dignity, and goals are just as important, which means adjuvant Osimertinib might not be the right choice for everyone. Without complete information it’s important to take the medical data available and apply it in the context of each patient. Through my advocacy work, I have learned that I cannot make my own culture, preferences, or beliefs the standard. Physicians must take steps outside of their comfort zone to try and understand what is meaningful to each patient, and together make a treatment decision.
I have several concerns surrounding endpoints, data, and whether prolonged exposure only delays or shortens the time to recurrence, and at what cost, literally and figuratively. I know many oncologists do as well, but the important part now is to step out of the scientific box and think about the vulnerable and scared person/patient, and their family, in front of you.
My Concerns as a Patient Research Advocate
- Adjuvant therapy is for curative intent after presumed curative treatment. There is a significant difference between outcomes of overall survival and disease-free survival, and as of now we only know that osimertinib can delay recurrence. Patients need to understand both when making a treatment decision. Osimertinib does not come without cost, literally and figuratively.
- Important questions will remain unanswered. Which patients have disease recurrence while taking osimertinib? Which will have recurrence after stopping therapy? Is there a pattern of recurrence? What are the resistance mechanisms, and should patients have chemotherapy first (I would!)? Those answers could provide the information needed to stratify patients who will benefit and avoid unnecessary harm to patients who are truly cured.
- Quality of life is extremely important, and side effects should not be minimized. “Tolerable” is relative to each patient. In addition, many patients do not fully disclose side effects to their health care team because they are worried about being taken off a treatment or trial, a dose reduction, or they are just determined and stubborn—like me. It should be noted here, as well, that it is too early to even understand long-term or late effects of treatment.
- It is not enough to develop new treatments if they will only benefit patients who have access to, and can afford, cutting edge care. We need cancer care and treatments that ALL patients can access.
My Lung Cancer Story, Including Osimertinib
My story started long before I was diagnosed. When I was 13, I had lost two grandparents to lung cancer within weeks of diagnosis and within weeks of each other. Six months after losing his own father, my dad was diagnosed with lung cancer, and he died three months later at the age of 41. There was a 10-year reprieve and then my mother’s sister was diagnosed with stage 1 lung cancer. She had surgery and was considered cured. Two years later, right before my wedding, they found another lung cancer on the other side. She had a lobectomy and was considered cured. Just two years after that my mom was diagnosed with lung cancer and died three months later at the age of 54. Less than a year after my mom died, my aunt developed a third lung cancer. Unfortunately, she didn’t have enough lung capacity to survive another surgery, so that lung cancer killed her one and a half years later.
In the 14 years between my dad being diagnosed with lung cancer and my mom’s diagnosis, there wasn’t a single advancement in lung cancer treatment, despite it being the number one cancer killer. In fact, twenty years ago, the only distinction doctors could make was whether a person had small cell or non-small cell lung cancer, and patients only had three treatment options: surgery, radiation, and/or chemotherapy.
I started getting periodic scans at age 27, when my mom was diagnosed with lung cancer. My scans were not concerning until 2009, when a nodule we had been following for three and a half years became aggressive, and I was diagnosed with lung cancer at 39 years old. I had surgery and was diagnosed with stage Ia adenocarcinoma, positive for an EGFR mutation (EGFR & KRAS were all they tested for).
At that time, there was some research regarding use of erlotinib as adjuvant therapy for patients with EGFR-mutated lung cancer after surgery. The clinical trial was on the East Coast, so I couldn’t participate, but I took erlotinib for 15 months off-label. I technically wasn’t even a candidate for adjuvant therapy, but I needed to be able to look my kids (who were 6, 8, 10, and 12) in the eyes and say that I did everything in my power. It was the only time in the past 11 years that I haven’t had cancer. Approximately eight months after I went off erlotinib, the cancer came back.
I had another surgery two and a half years later because the cancer was in a different area, and the doctors thought that it might be a new primary cancer. It was another EGFR-positive stage 1A lung cancer. But when I went for my first follow-up scan in January, there was another finding on the scan; when I went back in April, there were two more findings. At that point, they looked more closely at the two cancers that were resected and determined that it was the same EGFR cancer, but the only systemic therapy at that time was still erlotinib (they were just about to approve afatinib). Personally, the side effects I experienced from erlotinib were very quality-of-life inhibiting. Although there wasn’t any research at that time for using SBRT for intrapulmonary metastases, we used it on three unruly cancers. It allowed me to stay off systemic therapy for close to five years.
I had progression about two years ago and after a prudent discussion with my team, we all agreed that it was time I went back on systemic therapy, with osimertinib. The truth is that it really was the first time in the 10 years that I had been dealing with the disease that I was not overcome with fear. This was such a durable option, and I knew other promising therapies were in the pipeline, and I felt like I had the upper hand over the disease. Before this point, I had to keep erlotinib in my back pocket—there was nothing else. But now there was hope; osimertinib was now in the ‘toolbox’ of EGFR targeted therapies.
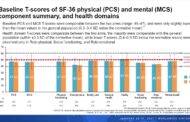
Patient-reported outcomes (PROs) are important, but when used in trials they are limited as it’s not a true representation of the lung cancer community. The problem with the PROs, and what concerns me, is that clinical trials do not represent real-world patients, because strict exclusion criteria prevent the majority of people with lung cancer in the real world from participating in trials. Real-world data, from real-world patients, should complement existing clinical and research data. The difference in reports of adverse advents is striking.
For coverage of findings related to ADAURA, read tomorrow’s edition of WCLC News, with highlights distributed daily and the full coverage distributed in an all-digital publication 2 weeks post-conference.
Excerpted from Finding Hope: A Patient’s Perspective on Adjuvant Therapy in Lung Cancer
Updated: Jun 13, 2020