While evidence-based indications for EGFR tyrosine kinase inhibitors (TKIs) exist for nearly all stages of EGFR-mutated non-small cell lung cancer (NSCLC), patients with unresectable stage III disease have not had access to these targeted therapies. This will likely change with the presentation of the primary results of the LAURA trial, which took place on June 1 during the 2024 American Society of Clinical Oncology (ASCO) Annual Meeting.
Suresh S. Ramalingam, MD, Professor of Hematology and Medical Oncology and Executive Director of Winship Cancer Institute at Emory University, Atlanta, drew applause from attendees after presenting the progression-free survival (PFS) data, which showed osimertinib treatment was associated with a statistically significant and clinically meaningful improvement in PFS following chemoradiotherapy of 39.1 months compared to 5.6 months with placebo with a hazard ratio of 0.16. (see Fig. 1) The 2-year PFS rate was 65% for patients in the osimertinib group and 13% for patients in the placebo group. Additionally, Dr. Ramalingam said these results were consistent across all key subgroups.
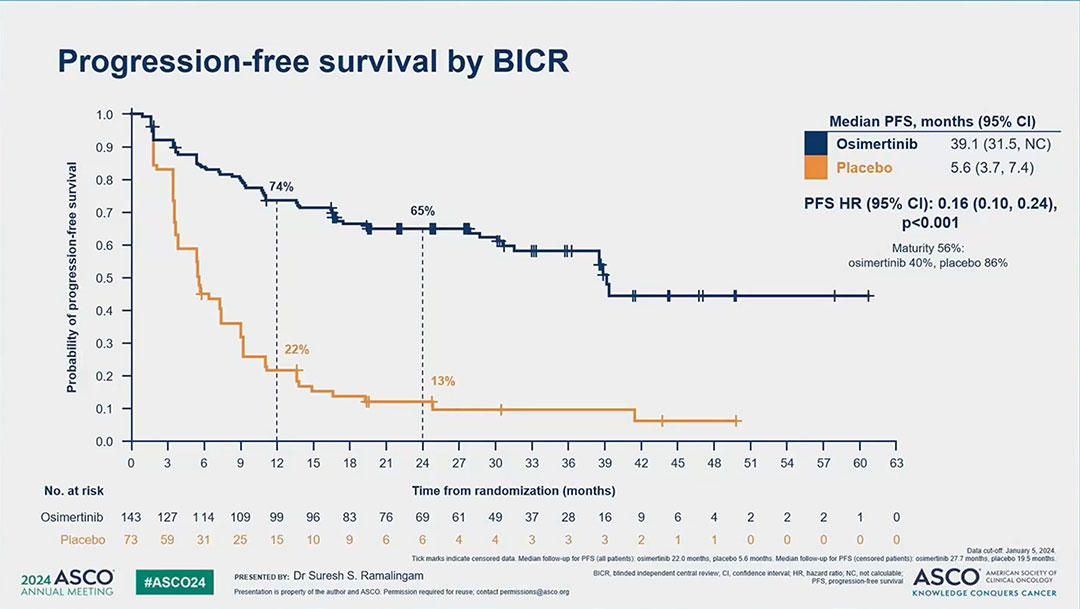
“We contend that EGFR-mutation testing is now critical for stage III patients to ensure optimal outcomes in the setting of EGFR-mutated lung cancer,” Dr. Ramalingam said. “Based on the strength of these data, we believe that osimertinib will become the new standard of care for patients with unresectable stage III EGFR-mutated non-small cell lung cancer after definitive chemoradiotherapy.”
The current standard of care for patients with stage III non-small cell lung cancer and unresectable disease is concomitant chemotherapy and radiation followed by immune checkpoint inhibition in the form of durvalumab for 1 year. However, as Dr. Ramalingam pointed out, recent evidence has shown that immune checkpoint inhibitors, given alone or in combination with chemotherapy, offer little benefit to patients with EGFR mutations. Indeed, a subset analysis from the PACIFIC trial showed no improvement in outcomes for EGFR-mutation positive patients who received durvalumab compared to the placebo group, though numbers were small.
With this in mind, Dr. Ramalingam said the LAURA study was a placebo-controlled trial conducted to evaluate the role of osimertinib—a third-generation EGFR TKI—for patients with locally advanced EGFR-mutated lung cancer following chemoradiotherapy. The study enrolled 216 patients who had completed chemoradiotherapy and not experienced disease progression.
Randomization occurred within 6 weeks of completion of chemoradiotherapy and patients with either exon 19 or 21 mutation were included. Patients were randomized 2:1 to either osimertinib or placebo, and treatments were continued until disease progression or unacceptable toxicity for patients. Baseline patient characteristics were similar between the two groups, though Dr. Ramalingam noted there were slightly more patients with a performance status of 0 (PS0) in the osimertinib group (56%) compared to the placebo group (42%).
At the database lock in January 2024, 90% of the patients in the placebo group had discontinued treatment—the vast majority due to disease progression, Dr. Ramalingam said. By comparison, in the osimertinib group, 44% had discontinued treatment. Of patients with centrally confirmed disease progression in the placebo group, 81% crossed over to receive post-protocol osimertinib therapy.
In terms of response, Dr. Ramalingam said the objective response rate and the disease control rate were higher for patients treated with osimertinib compared to placebo. The median duration of response was 36.9 months with osimertinib compared to 6.5 months with placebo. Additionally, the incidence of both local and distant metastases was lower for patients treated with osimertinib compared to placebo. Brain lesions were seen in 29% of the patients in the placebo group compared to 8% with osimertinib, Dr. Ramalingam said.
The overall survival data are only 20% mature to date, however, Dr. Ramalingam said at this point, the hazard ratio for overall survival is 0.81 favoring osimertinib, though the P value is not statistically significant. A full overall survival analysis will be performed when the data reach 60% maturity.

Discussant Lecia Sequist, MD, MPH, Program Director of the Cancer Early Detection and Diagnostics Clinic and Landry Family Professor of Medicine at Harvard Medical School, Boston, commended the trial’s effort for the high percentage of patients in the placebo group crossing over and receiving osimertinib.
“A key characteristic of patient centricity is ensuring access to therapy,” Dr. Sequist said. “In LAURA, the study protocol provided crossover osimertinib upon progression. Among the 73 patients randomized to placebo, 81% received crossover osimertinib. This high crossover rate exemplifies a tremendous effort by the study team, and, indeed, is better than many lung cancer clinical trials achieve. But it is still not 100%.
“However, relying on crossover and waiting until progression leaves some patients stranded because experiencing progressive lung cancer can fundamentally interfere with being fit enough to receive further treatment,” Dr. Sequist said. “Well, indeed, the LAURA PFS results we saw today strongly support consolidation osimertinib immediately—not waiting for progression—to maximize access and provide disease control.”
During her discussion, Dr. Sequist also supported the study designers’ decision to continue treatment indefinitely, citing the PFS as important for patients, particularly when progression in EGFR-mutant NSCLC may lead to a debilitating brain metastasis.
She said the biggest decision to note for LAURA is that study treatment continued indefinitely until progressive disease—a sharp contrast to all other trials ever done in stage III lung cancer, which have employed a finite course of therapy. She said she supported the decision to continue treatment indefinitely, citing the PFS as important for these patients, particularly when progression in EGFR-mutant NSCLC may lead to a debilitating brain metastasis.
However, indefinite treatment will undoubtedly spark questions about safety, cost, and quality of life.
In presenting the safety data, Dr. Ramalingam said the median duration of exposure to osimertinib was 24 months compared to 8.3 months with placebo, and grade 3 or higher events occurred in 35% of osimertinib-treated patients and 12% of patients in the control group.
“When we specifically look at treatment-related grade 3 or higher adverse events, they were 13% and 3% for the two groups, respectively,” he said. “Adverse events leading to drug discontinuation were observed in 13% in the osimertinib group and 5% for placebo. The most common toxicity observed was radiation pneumonitis for both groups of the patients. It was seen in 48% of osimertinib patients compared to 38% in the placebo group, and most were grade 1 or 2 in severity.”
Interstitial lung disease was reported in 8% of the patients in the osimertinib group. However, the majority were grades 1 and 2. There was one grade 5 event.
Dr. Sequist said there may be some patients for whom a 2- or 3-year course of osimertinib may offer a cure. The challenge will be finding those rare patients.
“There are defined, evidence-based approaches for trialing patients off TKIs. Frequent monitoring with an ultra-sensitive plasma assay that can reliably detect minimal residual disease is critical so that therapy can be reinstated, if necessary,” she said.
In lung cancer, however, Dr. Sequist said she believes assays are not yet sensitive enough to enable this approach.
“But technologies are advancing, and designing rational de-escalation trials for patients on the LAURA regimen should be a priority,” she said. “Ultimately, overall survival data, when mature, will help us decide about indefinite osimertinib. Given the data we saw today, I would personally already consider the LAURA approach for patients in my clinic with genetic alterations that have effective targeted therapies available which fit two additional criteria: the long-term side effect profile must be reasonable, and the drug must achieve good CNS penetration.”